
Treatment of Melasma with a 650-Microsecond, 1064-nm Laser and Microneedling
A Single-Center Retrospective Study by Dr. Ilaria Proietti
Background
Melasma is a chronic hypermelanosis characterized by hyperpigmented macules and patches on facial and sun-exposed areas, primarily affecting women and individuals with skin of color. Traditional topical treatments, including hydroquinone-based triple combinations, offer limited long-term success and are associated with adverse effects such as peeling, dryness, and uneven pigmentation. Energy-based devices, including Q-switched Nd:YAG and picosecond lasers, have been employed with varying efficacy, though they carry risks of postinflammatory hyperpigmentation (PIH), particularly in darker skin types. The 650-microsecond, 1064-nm pulsed Nd:YAG laser has demonstrated promise in preliminary small studies due to its low heat generation and reported safety across all Fitzpatrick skin types. Microneedling has also been explored as an adjunctive treatment, promoting collagen regeneration while preserving epidermal integrity, though larger-scale studies are needed to establish its efficacy in combination with laser therapy.
Objective
To evaluate the efficacy and safety of a 650-microsecond, 1064-nm pulsed Nd:YAG laser, administered alone and in combination with microneedling, for the treatment of facial melasma across diverse demographic subgroups.
Study Design / Materials and Methods
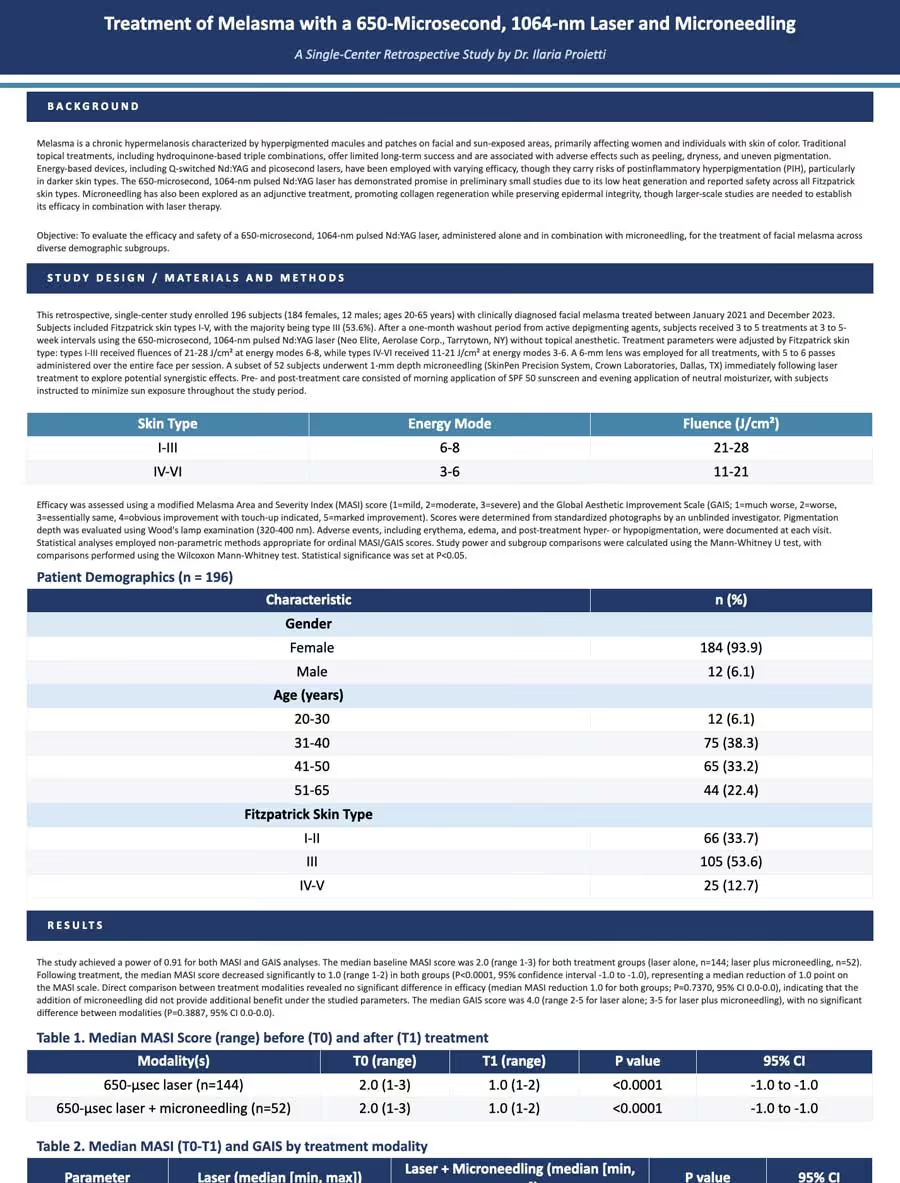
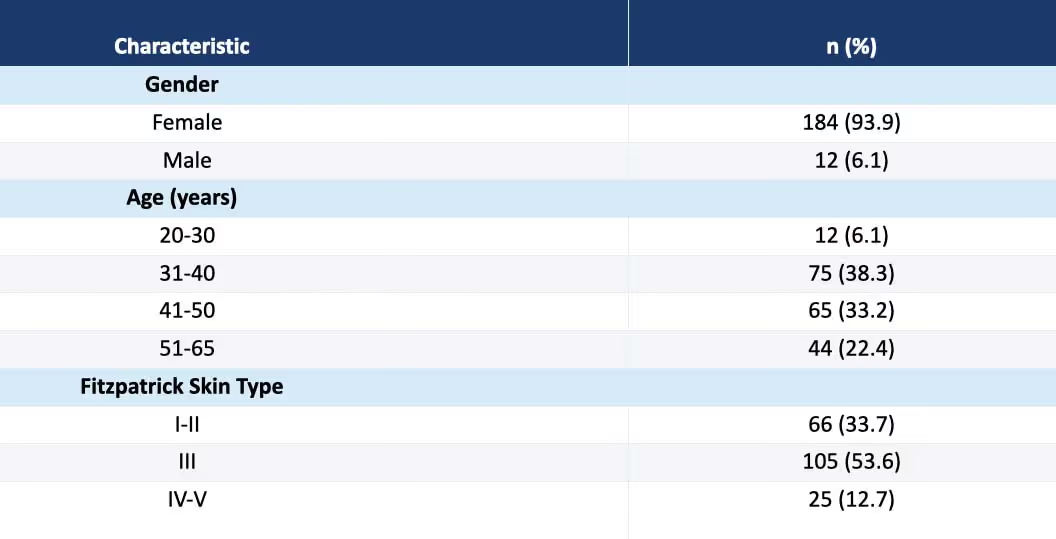
This retrospective, single-center study enrolled 196 subjects (184 females, 12 males; ages 20-65 years) with clinically diagnosed facial melasma treated between January 2021 and December 2023. Subjects included Fitzpatrick skin types I-V, with the majority being type III (53.6%). After a one-month washout period from active depigmenting agents, subjects received 3 to 5 treatments at 3 to 5-week intervals using the 650-microsecond, 1064-nm pulsed Nd:YAG laser (Neo Elite, Aerolase Corp., Tarrytown, NY) without topical anesthetic. Treatment parameters were adjusted by Fitzpatrick skin type: types I-III received fluences of 21-28 J/cm² at energy modes 6-8, while types IV-VI received 11-21 J/cm² at energy modes 3-6. A 6-mm lens was employed for all treatments, with 5 to 6 passes administered over the entire face per session. A subset of 52 subjects underwent 1-mm depth microneedling (SkinPen Precision System, Crown Laboratories, Dallas, TX) immediately following laser treatment to explore potential synergistic effects. Pre- and post-treatment care consisted of morning application of SPF 50 sunscreen and evening application of neutral moisturizer, with subjects instructed to minimize sun exposure throughout the study period.

Efficacy was assessed using a modified Melasma Area and Severity Index (MASI) score (1=mild, 2=moderate, 3=severe) and the Global Aesthetic Improvement Scale (GAIS; 1=much worse, 2=worse, 3=essentially same, 4=obvious improvement with touch-up indicated, 5=marked improvement). Scores were determined from standardized photographs by an unblinded investigator. Pigmentation depth was evaluated using Wood's lamp examination (320-400 nm). Adverse events, including erythema, edema, and post-treatment hyper- or hypopigmentation, were documented at each visit. Statistical analyses employed non-parametric methods appropriate for ordinal MASI/GAIS scores. Study power and subgroup comparisons were calculated using the Mann-Whitney U test, with comparisons performed using the Wilcoxon Mann-Whitney test. Statistical significance was set at P<0.05.
Patient Demographics (n = 196)
Results
The study achieved a power of 0.91 for both MASI and GAIS analyses. The median baseline MASI score was 2.0 (range 1-3) for both treatment groups (laser alone, n=144; laser plus microneedling, n=52). Following treatment, the median MASI score decreased significantly to 1.0 (range 1-2) in both groups (P<0.0001, 95% confidence interval -1.0 to -1.0), representing a median reduction of 1.0 point on the MASI scale. Direct comparison between treatment modalities revealed no significant difference in efficacy (median MASI reduction 1.0 for both groups; P=0.7370, 95% CI 0.0-0.0), indicating that the addition of microneedling did not provide additional benefit under the studied parameters. The median GAIS score was 4.0 (range 2-5 for laser alone; 3-5 for laser plus microneedling), with no significant difference between modalities (P=0.3887, 95% CI 0.0-0.0).
Table 1
Median MASI Score (range) before (T0) and after (T1) treatment

Table 2
Median MASI (T0-T1) and GAIS by treatment modality

Subgroup analyses demonstrated consistent efficacy across age groups and Fitzpatrick skin types. Age-stratified analysis (20-40 years [n=87, power 0.82], 41-50 years [n=65, power 0.85], and 51-65 years [n=44, power 0.84]) showed median MASI reductions of 1.0 across all age categories with no significant inter-group differences (P values ranging from 0.3546 to 0.8012). Similarly, Fitzpatrick skin type subgroup analysis (type II [n=66, power 0.94], type III [n=105, power 0.88], and types IV-V [n=25, power 0.84]) revealed median MASI reductions of 1.0 across all skin types without significant differences (P values ranging from 0.6589 to 0.8201). GAIS scores were similarly consistent across age groups (median 4.0 for all groups; powers 0.85-0.91) and skin types (median 4.0 for types II and III, 3.0 for types IV-V; powers 0.84-0.94), with no statistically significant differences between subgroups.
Table 3
MASI Scores (T0-T1): Median [min, max], P values, 95% CIs — Age Subgroups

Table 4
MASI Scores (T0-T1): Median [min, max], P values, 95% CIs — Fitzpatrick Skin Type Subgroups

Safety outcomes were favorable across all subjects. Treatments were well tolerated without procedural pain, and no subjects required topical anesthesia. Serious or unexpected adverse events were not observed. Notably, post-treatment hyperpigmentation or hypopigmentation — a significant concern with other laser modalities, particularly in skin of color — was not documented in any subject. Transient erythema, when present, resolved spontaneously without intervention. Patient satisfaction exceeded 85%, with the majority of subjects achieving GAIS scores of 4 or higher, indicating obvious to marked improvement in appearance.
Clinical Examples
Figures 1-3. Before (left) and after (right) photographs taken under standardized conditions using the Sylton® Diagnostic Systems device.
Figure 1
A 48-year-old female patient with Fitzpatrick skin phototype II presenting with facial melasma. Noticeable improvement is observed one month after the second monthly session using only the 650-microsecond, 1064-nm pulsed Nd:YAG laser.

Figure 2
A 43-year-old female patient with Fitzpatrick skin phototype III presenting with facial melasma. Noticeable improvement is observed one month after the third monthly session using only the 650-microsecond, 1064-nm pulsed Nd:YAG laser.

Figure 3
A 45-year-old female patient with Fitzpatrick skin phototype VI presenting with facial melasma. Noticeable improvement is observed one month after a single session using only the 650-microsecond, 1064-nm pulsed Nd:YAG laser.

Conclusions
This 196-subject retrospective study demonstrates that the 650-microsecond, 1064-nm pulsed Nd:YAG laser provides safe, significant, and reproducible improvements in facial melasma across diverse demographic subgroups, including various age ranges (20-65 years) and Fitzpatrick skin types (I-V). The treatment achieved statistically significant reductions in MASI scores (P<0.0001) with high patient satisfaction rates exceeding 85%. Importantly, the excellent safety profile — characterized by absence of procedural pain, no requirement for anesthesia or cooling, and complete absence of post-inflammatory hyperpigmentation — positions this modality as particularly suitable for patients with skin of color, a population historically at higher risk for PIH with conventional laser treatments.
The addition of microneedling immediately following laser treatment did not significantly enhance efficacy under the parameters studied, suggesting that the 650-microsecond laser alone may be sufficient for melasma treatment. The consistency of outcomes across age groups and skin types indicates broad applicability of this treatment protocol. The 650-microsecond pulse duration appears to offer distinct advantages over traditional millisecond-pulse Nd:YAG lasers and Q-switched systems, likely attributable to reduced heat generation and thermal diffusion to surrounding tissues, thereby minimizing the risk of melanocyte stimulation and subsequent PIH.
These findings expand upon limited prior reports (Johnson et al., 2020, n=3; Greywal and Ortiz, 2021, n=10) and provide more robust evidence for the efficacy and safety of 650-microsecond, 1064-nm laser therapy in melasma management. The treatment protocol's advantages include: (1) no requirement for topical anesthesia or skin cooling, enhancing patient comfort and clinical workflow efficiency; (2) safety across all treated Fitzpatrick skin types without post-treatment pigmentary complications; (3) minimal downtime with resolution of transient erythema within hours; (4) consistent efficacy regardless of patient age or skin type; and (5) high patient satisfaction with realistic aesthetic improvements.
Study limitations include the retrospective design, single-center setting, absence of a control group, evaluation by an unblinded investigator (introducing potential bias), and limited long-term follow-up data regarding recurrence rates. Future prospective, randomized, double-blind, multicenter trials with extended follow-up periods are warranted to confirm these findings, establish optimal treatment parameters for different melasma subtypes (epidermal, dermal, mixed), evaluate long-term recurrence rates, and directly compare the 650-microsecond laser with other established treatment modalities such as Q-switched Nd:YAG, picosecond lasers, and combination topical therapies.
In conclusion, the 650-microsecond, 1064-nm pulsed Nd:YAG laser represents a promising, safe, and effective treatment option for facial melasma that addresses the limitations of traditional therapies while offering particular advantages for patients with skin of color. The technology merits consideration as a valuable addition to the therapeutic armamentarium for this challenging and psychosocially impactful dermatologic condition.

1064nm Nd:YAG Laser with a short 650-microsecond pulse duration for the treatment of dyschromia and skin tightening
Six patients seeking improvement in dyschromia and skin laxity were enrolled to evaluate the safety and efficacy of the 1064nm Nd:YAG 650-microsecond laser.

1064nm Nd:YAG Laser with a 650ms Pulse Duration for the Treatment of Melasma: A Clinical Evaluation
We aim to evaluate the efficacy and safety of the 1064nm Nd:YAG laser with a 650-microsecond pulse duration for the treatment of melasma.